Looking to the Horizon of Glioblastoma Treatment

By Jaanu
Know thine enemy and know thyself, said Sun Tzu. Even if you fight a thousand battles, you’ll tally up a thousand victories.
Biomedical research took this principle to new heights with the dawn of the genomics era. Uncovering molecular mechanisms (how proteins and other molecules interact to cause or catalyze disease) and genetic landscapes (mutations and modifications to the genetic code) of any given disease offers opportunities for new therapeutic targets. In other words: know thine enemy, and you know what drug targets are going to go right to the source.
Despite leaps in medical innovation, the brain cancer field is still fraught with landmines. In 1947, John Gunther’s son died of a glioma. Gunther wrote the gut-wrenching memoir Death Be Not Proud to capture his son’s legacy in some way. 80 years later glioblastoma is still the most  aggressive and lethal brain cancer in adults. But much has changed, giving us much cause for hope, as well. Imaging has improved immensely, allowing more precise, more thorough surgical resection of brain tumors. Research into immunotherapies has improved, and patients are beginning to respond better to such treatments.
aggressive and lethal brain cancer in adults. But much has changed, giving us much cause for hope, as well. Imaging has improved immensely, allowing more precise, more thorough surgical resection of brain tumors. Research into immunotherapies has improved, and patients are beginning to respond better to such treatments.
People say that every type of cancer should be considered a distinct disease. This certainly seems to hold true for glioblastomas and other brain tumors. The genetics of meningiomas, or tumors of the meninges (thin layers of tissue covering the brain), are very different from the genetics of choroid plexus tumors (which haunt the network of blood vessels and cells in the brain’s ventricles). Tumors which metastasize to the brain are an entire subspecialty of neuro-oncology— and they have their own unique genetic signatures.
The research in this article comes from a 2025 review on the current body of glioblastoma research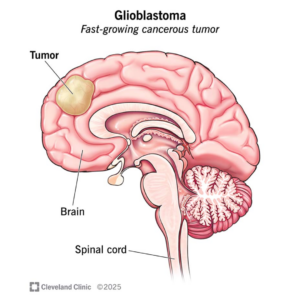 by Dr. Gatikrushna Singh and his active team at the University of Minnesota.
by Dr. Gatikrushna Singh and his active team at the University of Minnesota.
Firstly, what is glioblastoma, and why is it so dangerous? It is a tumor comprised of glial cells from the central nervous system. It’s an irritatingly invasive tumor, because glial cells can be found working hard all across the brain, and is also very resistant to conventional chemotherapies (chemical treatments). One reason is the high presentation of the EGFR gene in glioblastoma cells. EGFR, or epidermal growth factor receptors, signal the cell to continue growing and dividing. Overexpression of these receptors sends constant growth signals and the cell multiplies uncontrollably. Glioblastoma cells also have longer lifetimes because of a few other abnormalities. Another reason it’s so hard to treat is that the cells within a single tumor are very heterogeneous. This means that just targeting one type of tumor cell won’t eliminate the problem even if it causes a remission in the cancer type.
Some good news, though, is that solid, or circumscribed glioblastomas tumors, have a better prognosis than ever before. Advanced imaging techniques makes surgical resection of these tumors quite successful. Unfortunately, glioblastoma can also be highly invasive and infiltrative. This poses a massive challenge for surgical intervention.
What can we begin to do about a cancer this complex?
First is molecular characterization of the disease. Treating every patient as if their disease is the same is an ineffective approach to cancer treatment, according to Dr. Nic Jones, formerly of the Manchester Cancer Research Centre. Molecular characterization permits the “subtyping” of the disease – breaking it down into different tumor classes which are susceptible to different treatment approaches. For example, “proliferative GBM” is a cancer class that reveals high levels of TOP2A and PCNA, markers which can then be used as targets for therapies. As shown in the image here, biomarkers can be on the inside or surface of the cell.
same is an ineffective approach to cancer treatment, according to Dr. Nic Jones, formerly of the Manchester Cancer Research Centre. Molecular characterization permits the “subtyping” of the disease – breaking it down into different tumor classes which are susceptible to different treatment approaches. For example, “proliferative GBM” is a cancer class that reveals high levels of TOP2A and PCNA, markers which can then be used as targets for therapies. As shown in the image here, biomarkers can be on the inside or surface of the cell.
Aside from using improved molecule-level methods for biomarker detection and classification, improved imaging techniques, like proton MR spectroscopy and MRI/PET scanning, are valuable in the clinic, especially in assessing tumor progress and having diagnostic applications.
The main challenges to navigate when it comes to improving survival rates are tumors which develop resistance to therapies or which recur even after surgical resection or other treatments. However, new approaches are being developed in labs around the world at a very rapid rate. Better knowledge of GBM subtype-specific biomarkers has launched new targeted therapies, like inhibition of Epidermal Growth Factor Receptors. Immunotherapies like CAR-T cell therapies use patients’ own powerful immune cells to fight tumors with high specificity.
Today, glioblastoma has a median survival rate of just over 1 year. The promise of progress to come means there is still a lot of work to be done. As I continue to write for Spirit in medical school and beyond, I’m dreaming of a follow-up to this article: one describing more strategies for early detection, longitudinal studies on effective immuno- and surgical therapies— and high, high rates of complete cures. 🧠


